Pain after a hip fracture? Finding out why
Approximately 350,000 people fracture their hips each year in the US. Most but these injuries occur in people over 60 due to a fall. Unfortunately, this number will grow with each year as our population ages. The hip refers to the ball-and-socket joint that connects our pelvis to our thigh bone. A “hip fracture” is a break in the upper part of thigh bone. This fracture can occur inside the hip joint capsule, “intra-articular” or outside, “extra-articular”.
When someone breaks their hip, it is considered a medical emergency and almost always, surgery is recommended. The type of surgery needed depends on where in the femur the fracture occurred, and if the fracture is displaced and how much. The most appropriate surgery is also decided based on the prognosis of the fracture healing and producing a good result, the person’s age and their activity level. A fracture that occurs just below the ball of the hip and is displaced, is inside of the hip joint capsule and often does not heal and produce a good result. As a result, often this fracture is treated by replacing the femoral head (partial or bipolar hip) or the entire hip (total hip replacement) with a prosthesis rather than try to fix the fracture. In a young patient with a femoral neck fracture, more often an attempt may be made to preserve or salvage their own hip by fixing the fracture, in spite of the increased chance this attempt will fail and more surgery will be needed. The hope was to stave off the need for a hip replacement in someone very young.
Patients who are treated with a replacement often recover more quickly than patients whose hip fracture is repaired, but not always. The advantage of replacing the ball when there is a fractured neck (partial hip) or the whole hip (total hip) rather than trying to get the bone to heal is that it’s more predictable and more often produces a better result. The implanted prosthesis, however, must be stable against skeleton (not loose), appropriately sized and positioned to recreate equal leg lengths and normal hip mechanics. The soft tissues which surround the hip, including the nerves, must be preserved and respected. Very importantly, infection must be prevented. If these conditions don’t happen, then often the result is not good and that person is not happy. If you can figure out what went wrong such as a loose hip stem or an underlying infection, then hopefully the condition can be corrected.
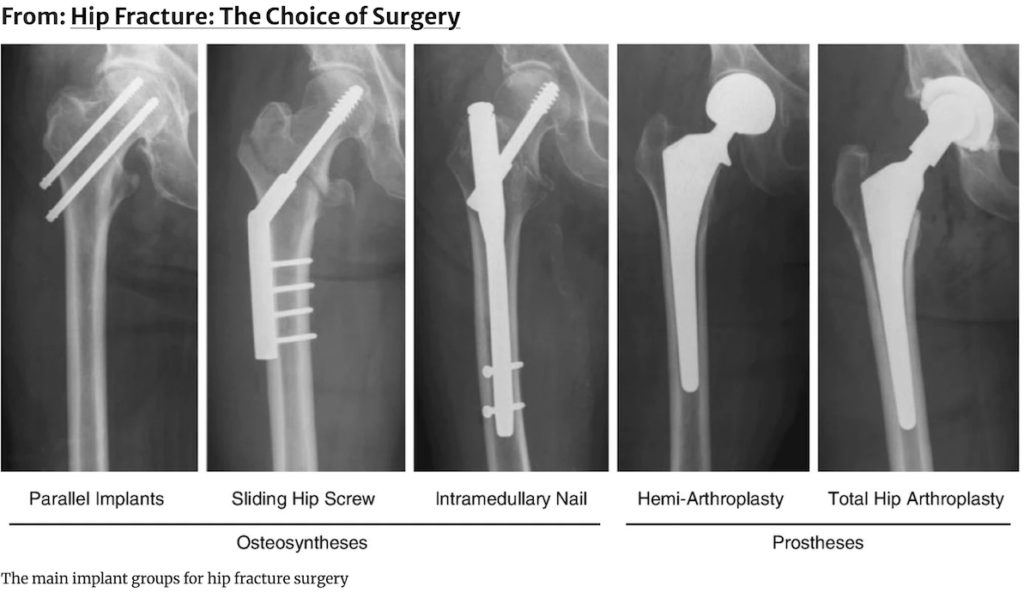 The above image is created by Henrik Palm and published by Springer Nature.
The above image is created by Henrik Palm and published by Springer Nature.
When the break occurs below the hip joint capsule or through the femoral neck but with minimal or no fracture displacement, then a decision may be made to internally fix the fracture hoping it will heal. The surgeon “reduces the fracture” attempting to return the broken pieces of bone back to the position they were in prior the fracture and then “internally fixes” the fracture by implanting metal hardware hoping to hold the fracture in that position. For femoral neck fractures, 2 or 3 screws are inserted across the fracture and into the femoral head to fix the fracture. For fractures that occur below the hip joint capsule, a rod or “nail” is inserted down the medullary canal of the femur and a thick screw (lag screw) is inserted into the femoral head through a hole in the “nail” to hold the fracture. Depending on the fracture, the “nail” will extend to just above mid-thigh level or all the way down to the knee. One or two screw is then inserted through holes in the bottom of the “nail”. Surgeons also fix these fractures with a bone plates fixed to the side of the upper femur with multiple screws and a large screw inserted through the plate and into the femoral head.
In order for a fracture to heal, the broken bone fragments must be opposed to each other and subjected to compression. Each type of hardware described above allows for the fracture to compress together. Walking after the surgery is important to compress the fracture and stimulate healing. Sometimes, full weight bearing must be delayed due the complexity of the fracture and the stability of the internal fixation.
Unfortunately, sometimes the fracture reduction and internal fixation is not stable enough and the fracture collapses. The fragments can heal in this collapsed position or not. Patients sometimes complain that their leg has become short and turns out. Fracture fragments that don’t heal sometimes are painful with movement and weight bearing. The collapse of the fracture can also result in impingement of the healed boney fragments against the socket or pelvis causing pain. The hardware which was implanted to hold the fracture occasionally “cuts out” of the bone as it collapses which can irritate or destroy tissue and cause pain.
The femoral head has a precarious blood supply. Often the blood supply is destroyed in a femoral neck fracture. When a decision is made “pin” or “internally fix” this fracture, the assumption and hope is that the blood supply is still intact the facture can heal. Sometimes the fracture does not heal resulting in pain and disability. Sometimes the femoral neck fracture does heal but the blood supply to the head is not adequate and bone that makes up the head dies and later collapses. This condition is referred to as avascular necrosis or AVN. The “pins” or screws inserted into the head can then poke into the socket destroying cartilage and cause arthritis and pain. The “pins” can also protrude out of the side of the hip as the fracture compresses together causing tissue irritation and pain.
Fortunately, most people who break their hip and are treated with surgery do well. If you are not doing well, then if the exact reason why is understood, then hopefully a strategy can be developed to correct it.
Check out Dr. Leone’s Patient Testimonials. These grateful patients make it all worthwhile.
The Leone Center for Orthopedic Care at Holy Cross Hospital is located at 1000 NE 56th Street in Fort Lauderdale. For more information or to schedule a consultation please call 954-489-4575 or visit holycrossleonecenter.com



